Harmonizing Healthcare Data Standards: The Role of USCDI, OHDSI, and Common Data Elements

Healthcare’s digital transformation has unlocked unprecedented potential for innovation, yet the promise of seamless data exchange remains hindered by a cacophony of incompatible systems and fragmented standards.
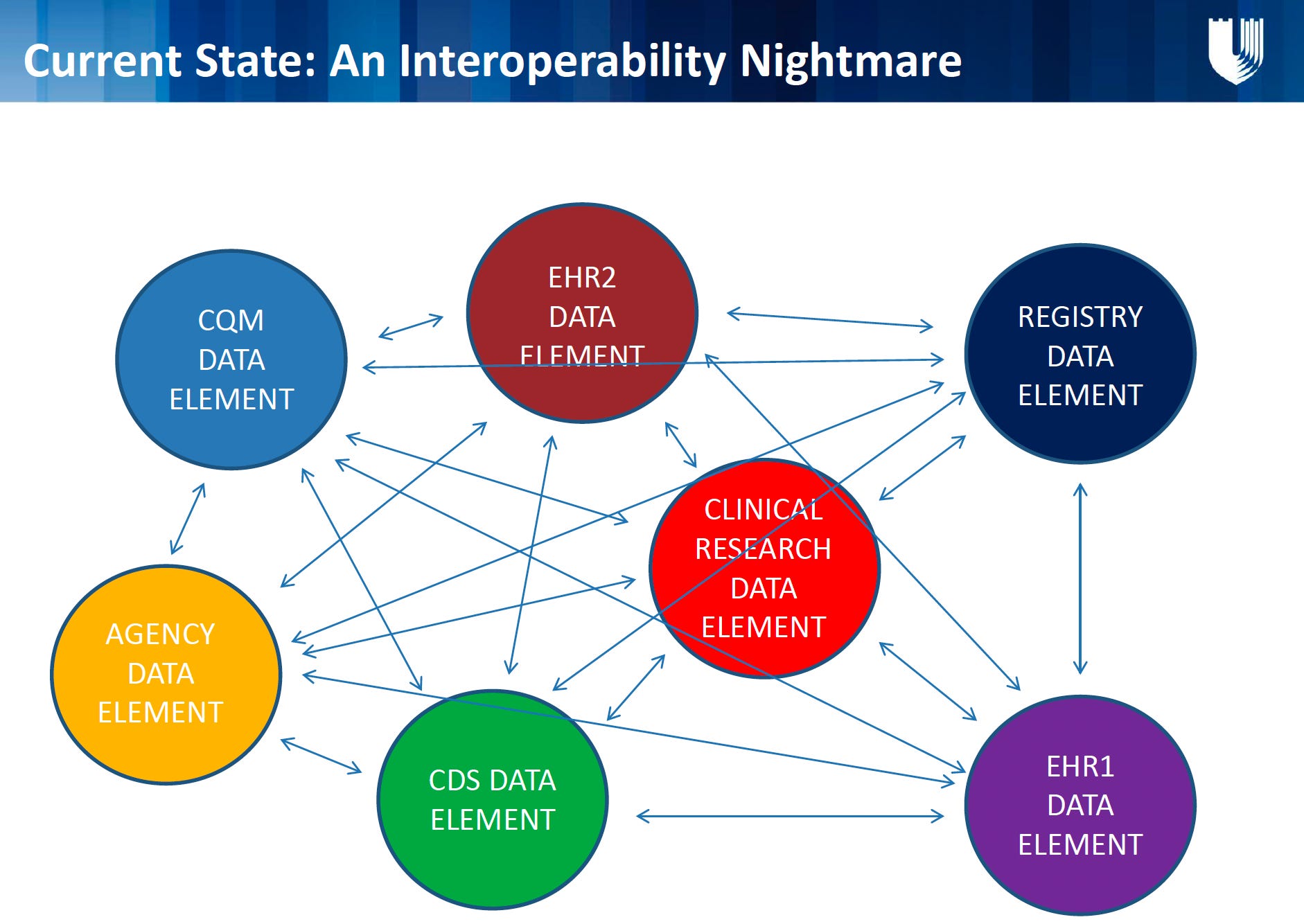
The diagram below, from the work of Duke Health and the Pew Charitable Trust, illustrates a complex web of disconnected EHRs, registries, and agencies. It highlights a crucial reality: without standardized data harmonization, the advancement of healthcare’s data revolution will be hindered.
Enter initiatives like the United States Core Data for Interoperability (USCDI), OHDSI (Observational Health Data Sciences and Informatics), and Common Data Elements (CDEs). These frameworks are the keys to transforming chaos into cohesion. Let’s explore their roles and the path to a unified future.
The Problem: A Tower of Babel in Healthcare Data
The diagram’s tangled web of EHRs, registries, and agencies underscores three core challenges:
Inconsistent Definitions: A “blood pressure” entry in EHR1 might differ from EHR2 or a research registry, leading to mismatched analyses.
Siloed Objectives: Clinical research, quality reporting (CQM), and public health agencies collect similar data but in incompatible formats.
Redundant Efforts: Systems like EDS DATA warehouses often duplicate work to reconcile disparities, wasting time and resources.
Without standardization, stakeholders operate in parallel universes—generating data that cannot be compared, aggregated, or leveraged at scale.
The Solution: Harmonizing Standards
1. USCDI: The Foundation of Interoperability
The United States Core Data for Interoperability (USCDI) is the U.S. government’s answer to fragmentation. This standardized dataset defines classes (e.g., “Clinical Notes,” “Allergies”) and specific elements (e.g., “Diastolic Blood Pressure”) that all certified health IT systems must support.
Impact: By mandating USCDI adoption (via the 21st Century Cures Act), EHRs like EHR1 and EHR2 can now share a common vocabulary, ensuring that a “medication list” in one system aligns with another.
Future Potential: Expanding USCDI to include social determinants of health (SDOH) and patient-generated data will create richer, more holistic records.
2. OHDSI and OMOP: Unlocking Large-Scale Analytics
The OHDSI initiative and its OMOP (Observational Medical Outcomes Partnership) Common Data Model tackle standardization for research and analytics. OMOP transforms disparate data sources—EHRs, claims, registries—into a consistent structure.
Impact: Researchers can run federated analyses across global databases (e.g., comparing treatment outcomes for diabetes in the U.S. vs. Europe) without manual harmonization.
Synergy with USCDI: While USCDI ensures baseline interoperability, OMOP enables advanced analytics—bridging the gap between care delivery and research.
3. Common Data Elements (CDEs): The Research Backbone
CDEs are standardized definitions (e.g., “pain severity scale”) used in clinical studies to ensure consistency. Organizations like NIH and NCI curate CDE libraries for conditions ranging from cancer to mental health.
Impact: Aligning CDEs with USCDI and OMOP allows research data (e.g., CLINICAL RESEARCH DATA) to flow seamlessly into EHRs and population health tools.
Example: A depression study using NIH’s CDEs could automatically integrate findings into a clinic’s EHR decision-support system.
4. FHIR: The Delivery Mechanism
Though not a standard itself, FHIR (Fast Healthcare Interoperability Resources) provides the modern API framework to operationalize USCDI, CDEs, and OMOP. FHIR resources can map data elements across systems, turning theoretical standards into real-world workflows.
The Roadmap: From Theory to Practice
1. Adopt USCDI as the Baseline
Providers and vendors must prioritize USCDI compliance, ensuring core data elements are consistently captured and exchanged.
Advocate for expanding USCDI to include genomics, SDOH, and patient-reported outcomes.
2. Integrate OHDSI/OMOP into Health IT Ecosystems
Health systems should map EHR data to OMOP to participate in collaborative research.
Payers and regulators could mandate OMOP-formatted submissions for real-world evidence generation.
3. Align CDEs with Regulatory and Clinical Needs
Harmonize NIH CDEs with USCDI to reduce research-to-practice translation barriers.
Develop tools that auto-convert CDE-based research data into FHIR resources for EHR integration.
4. Foster Public-Private Collaboration
ONC, NIH, and industry partners must co-design governance models for evolving standards.
Pilot projects (e.g., embedding OMOP into state health information exchanges) can prove scalability.
5. Educate and Incentivize Stakeholders
Train clinicians on the value of standardized data entry.
Offer grants or penalties to accelerate compliance, mirroring CMS’s Promoting Interoperability Program.
The Vision: A Symphony of Data
Imagine a world where:
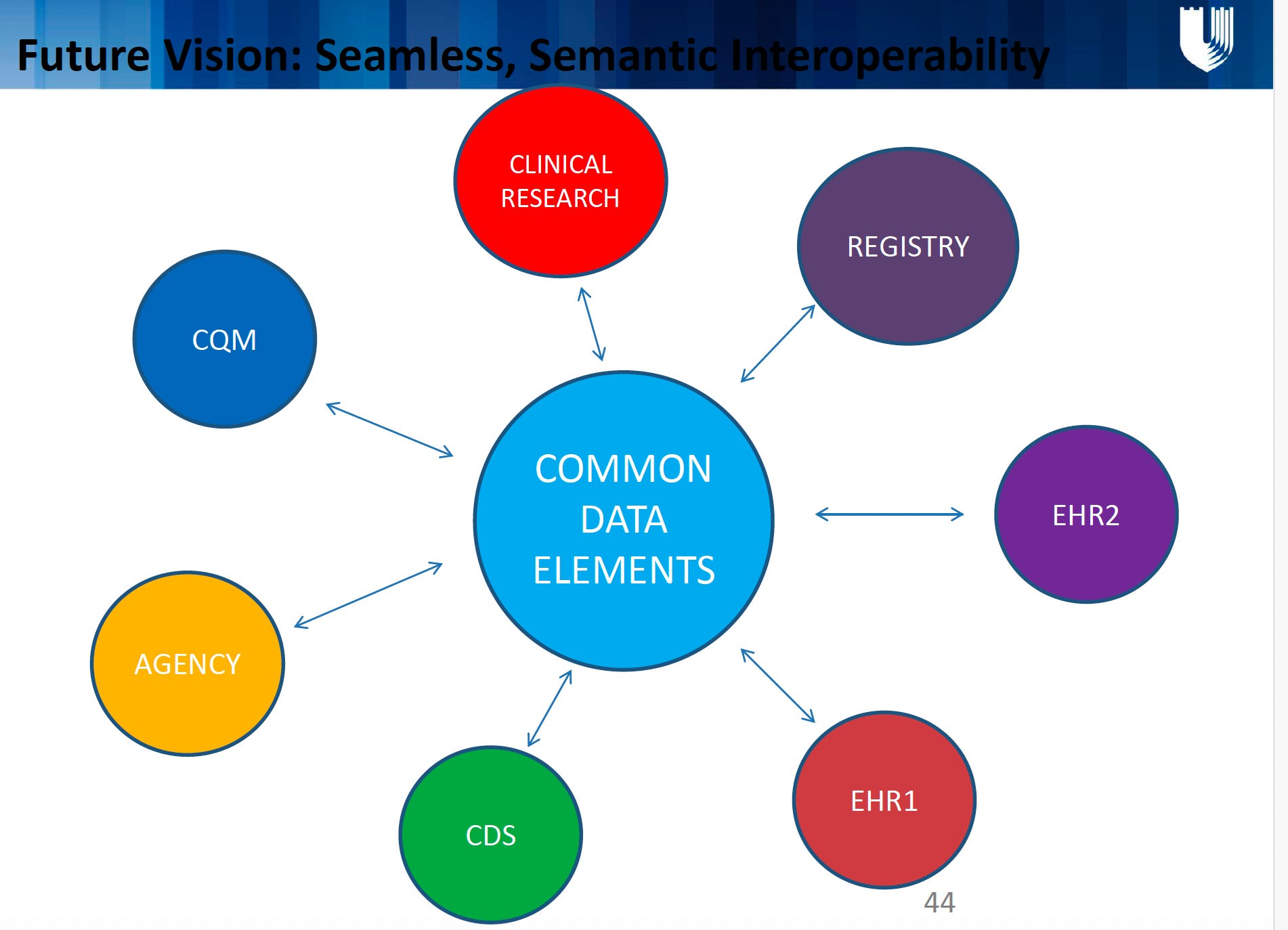
A clinician pulls up a patient’s record, seamlessly viewing USCDI-standardized data from multiple EHRs, enriched with OMOP-mapped research insights.
A public health agency detects a rare adverse drug event in days—not years—by analyzing OMOP-formatted data across hospitals.
A researcher combines CDE-based trial data with real-world EHR data to personalize cancer therapies.
This is the power of harmonized standards: data that is interoperable, reusable, and purposeful.
Conclusion
The diagram’s “interoperability nightmare” isn’t inevitable—it’s a symptom of uncoordinated progress. By rallying around USCDI, OHDSI, and CDEs, we can replace today’s chaos with clarity. The goal is not just standardization for its own sake, but a future where data flows effortlessly to improve care, accelerate discovery, and empower patients. Let’s stop reinventing the wheel and start building highways.